


Shoulder specialist in Bangalore is a technique that orthopedic specialists use to assess, analyze, and fix issues inside a joint. The word arthroscopy originates from two Greek words, “arthro” (joint) and “skopein” (to look). The term truly signifies “to peer inside the joint.” During shoulder arthroscopy, the specialist embeds a little camera, called an arthroscope, into your shoulder joint. Pictures from the camera are shown on a screen, which your specialist uses to treat the pathology inside the shoulder joint.
Since the arthroscope and careful instruments are slender (like a pencil), your specialist can utilize extremely little cut openings, instead of the bigger entry points (cuts) required for a standard, open medical procedure. This outcome in less agony for patients and abbreviates the time it takes to recoup and come back to most loved exercises. Despite the fact that shoulder arthroscopy has been performed since the 1970s, late advances have made it increasingly solid and powerful. It has made a finding, treatment, and recuperation from medical procedure simpler and quicker than was once suspected conceivable.
The shoulder joint is a mind boggling joint and is the most versatile joint in the body. It resembles a ball and attachment and is made of three bones: It is comprised of three bones: your upper arm bone (humerus), your shoulder bone (scapula), and your collarbone (clavicle). Ball and attachment: The upper finish of the arm bone (humeral head) fits into an adjusted attachment (glenoid) in your shoulder bone. Both the articulating surfaces are secured by a dangerous tissue called articular ligament. It makes a smooth, frictionless surface that enables the unresolved issues effectively over one another. The glenoid is lined by a solid sinewy ligament called the labrum. The labrum structures a gasket around the attachment and extends it, includes steadiness, in this way lessening the opportunity of disengagement (ball sneaking out of the attachment).
Shoulder case: for the shoulder to function admirably, the bones need to remain together. The joint container holds the ball and attachment together. The joint is encompassed by groups of tissue called tendons. They structure a case that holds the joint together. The undersurface of the case is lined by a slim film called the synovium. It produces a synovial liquid that greases up the shoulder joint.
Rotator cuff: Four tendons surround the shoulder capsule and help keep your arm bone centered in your shoulder socket. This thick tendon material is called the rotator cuff. The cuff covers the head of the humerus and attaches it to your shoulder blade.
Bursa: There is a lubricating sac called a bursa between the rotator cuff and the bone on top of your shoulder (acromion). The bursa helps the rotator cuff tendons glide smoothly when you move your arm.Shoulder specialist in Bangalore,Shoulder arthroscopy Bangalore
You may need Shoulder arthroscopy Bangalore if you have a painful condition of the shoulder that is not responding to non – surgical treatment. Non surgical treatment includes pain medications, exercises and physiotherapy and injections. You may also need arthroscopy for recurrent shoulder dislocations and for some shoulder injuries that are caused by trauma or overuse.
Common arthroscopic procedures include:
- Rotator cuff repair
- Bone spur removal
- Removal or repair of the labrum
- Repair of ligaments
- Removal of inflamed tissue or loose cartilage
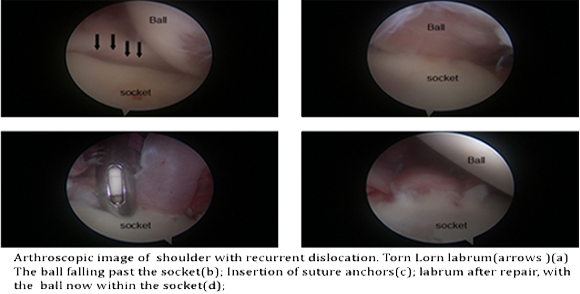
- Repair for recurrent shoulder dislocation
- Certain procedures like nerve release, cyst excision

Advantages of shoulder arthroscopy:

With arthroscopy being used more frequently for different conditions, the recovery has been quicker and surgeries have been less painful. The scars are small and most surgeries are now day care procedures. In addition arthroscopy has made visualization of problems more easier and effective as the surgeon can examine every nook and corner of the joint with the camera.
Most shoulder arthroscopies are day care procedures, however your surgeon may advice admission for a day or two depending on your condition. Before the surgery you may be needed to consult your anaesthetist to ascertain the fitness for surgery.
Anaesthesia:
You are given a general anaesthesia most of the times, with an injection (block) in your neck. This injection helps pain control following surgery and may cause temporary numbness and weakness of your upper limb and fingers following surgery. It usually recovers in a few hours.
Surgical procedure:
Once you are anaesthetised, you will be positioned appropriately. Small puncture holes (usually between 2-4) are done around the shoulder joint. One of the holes will be used to insert a camera (the arthroscope) which is used to visualise the joint. The joint will be filled with saline to aid visualization. The other holes are used to insert instruments (which are as thin as a pencil) to repair the tissues or to remove unwanted tissues.

Once the procedure is completed, the portals (holes) are closed and dressing is applied. Your arm will be placed in a bag (sling/ brace). You will need to wear the sling for a few weeks depending on what procedure you are having.
After surgery:
Even though recover is faster when compared to open surgeries, you will need to follow your surgeon’s advice. you can go home the same day or the day after surgery depending on your surgeon’s advice. You will have small dressings, the care of which will be instructed to you. Instructions regarding your sling/ brace will also be given. You are not allowed to drive until approved by your surgeon. You will be given pain medications to help relieve pain for the first few days. Icing will also help relieve pain. Although it does not affect how your shoulder heals, lying flat may pull on your shoulder and cause discomfort. Some patients are more comfortable sleeping in a reclining chair or propped up in bed during the first days after surgery.
Rehabilitation:
Rehabilitation plays an important role in getting you back to your daily activities. An exercise program will help you regain shoulder strength and motion. Your surgeon will develop a rehabilitation plan based on the surgical procedures you required.
If you have had a more complicated surgical repair, your surgeon may recommend a physical therapist to supervise your exercise program.