

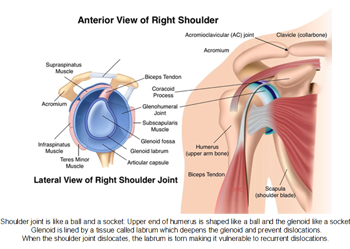
The shoulder is the most moveable (adaptable) joint in our body. It causes you to lift your arm, to turn it, and to reach up over your head. It can turn in numerous ways. This more noteworthy scope of movement, which is absent in some other joint can be that as it may make the shoulder vulnerable to disengagements. Shoulder insecurity (disengagement) happens when the leader of the upper arm bone is constrained out of the shoulder attachment. This can occur because of unexpected damage or abuse.
When a shoulder has disjoined, it is defenseless against rehash scenes. At the point when the shoulder is free and sneaks out of spot over and over, it is called interminable shoulder unsteadiness. Our shoulder joint resembles a ball (the upper finish of the humerus bone) and attachment (glenoid). The ball is bigger than the attachment. This makes our shoulder is the most adaptable joint in the body, enabling you to toss balls, lift overwhelming articles and connect practically any way. The labrum is a ring of extreme and adaptable tissue on the edge of the glenoid. It appends the glenoid to the container and makes the glenoid attachment more profound, consequently making shoulder separation more outlandish.
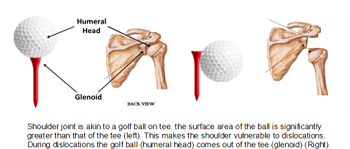 Shoulder disengagement happens when the ball is mightily determined out of the attachment. On the off chance that the humeral head moves totally off the glenoid, this is known as a disengagement. The most widely recognized reason for shoulder separation is shoulder damage. Falling or running into something, a brandishing tackle or lifting something far can overstretch your shoulder joint.
Shoulder disengagement happens when the ball is mightily determined out of the attachment. On the off chance that the humeral head moves totally off the glenoid, this is known as a disengagement. The most widely recognized reason for shoulder separation is shoulder damage. Falling or running into something, a brandishing tackle or lifting something far can overstretch your shoulder joint.
A patient with instability usually has a history of injury, which caused the shoulder to dislocate. Following this episode, the shoulder can dislocate again and again, either partial or completely. These episodes can happen after a trivial injury to the shoulder, during playing or during activities of daily living or sometimes even during sleep.
The treatment of shoulder instability is to get your shoulder back under control and ensure it does not dislocate again and again.In some patients this can be achieved by a physiotherapy program and in others it will involve an operation.
Treatment depends on your age, activity level and type and direction of instability. Physiotherapy can help restore stability, strength and control of your shoulder. It helps you regain control of the rotator cuff and other shoulder muscles – and training them to take over from the parts of the shoulder that are damaged and are no longer doing their job. There are some types of instability where physiotherapy alone is enough to stabilise the shoulder, where as in some, surgery is essential to achieve stability of the shoulder. The operation is also sometimes necessary because each time the shoulder dislocates more damage is done to the joint itself and this might increase the risk of arthritis in the future.
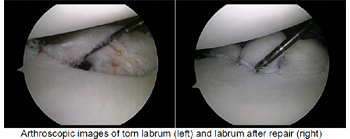
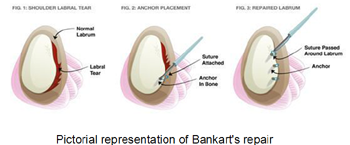
Surgery helps restore shoulder stability by tightening and repairing the labrum and the capsule.
There are several different techniques available to stabilise your shoulder.
The arthroscopic procedure (key hole surgery) has excellent results in cases where there have been few dislocations. This operation has a success rate of about 90%. The advantages of arthroscopic surgery includes shorter hospital stay, less pain, smaller scars. The principles of the operation are to reduce the size of the stretched capsule of the shoulder joint and to reattach the torn labrum back to the bone. You will have two or three small holes at the back and front of your shoulder. The camera is inserted thorough one of the holes. The other holes are used for instrumentation. Pencil thin instruments are introduced and the labrum, or cartilage, which is torn off the bone and is repaired with a screw which has stitches attached to the end (suture anchors). Success Story: Shoulder Dislocation

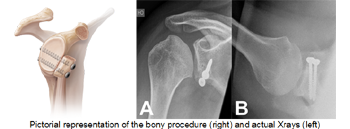
The open operation (latarjet procedure):
Commonly known as a “full reconstruction”has a higher success rate especially in people who have had several dislocation over many years or who are very active and play elite contact sport. The success rate of the open operation is greater than 95%. The open operation is preferable when there has been significant bony damage as it allows for bone grafting procedures to be performed.
It involves a cut in front of the shoulder. The coracoid bone is cut along with its muscle attachments and fixed in front of the glenoid bone to increase the stability of the shoulder and prevent the ball from dislocating.
What happens after the operation?
Following the operation, you will have your arm placed in the sling.The sling will need to remain on for at least 4 weeks. At about 10 days after surgery you will be seen to take out your stitches and check that the wound is clean and that there is no infection. You will again be reviewed at the 4 week mark, to be taken out of the sling and start an exercise program.
At about 6 months, providing you have sufficient muscle control of the shoulder, you will be permitted to resume full activity, including contact sports. You will however need to continue the exercise program for at least 9 months following surgery. Your shoulder may be a little stiff for up to 12 months following surgery.Success Story : Shoulder Dislocation