

Simply defined, arthritis is inflammation of one or more of your joints. Arthritic shoulder can be the cause of pain and stiffness during your activities of daily living.
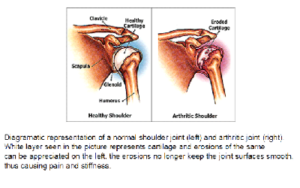
Your shoulder is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
The head of your upper arm bone fits into a rounded socket in your shoulder blade. This socket is called the glenoid. The bones never come in contact with each other. This is due to the presence of a smooth slippery substance on the inside of each bone, which acts like a cushion. It is called cartilage.
The inside of the joint is lined by a thin membrane called the synovial membrane. This membrane releases a fluid that lubricates the cartilage and reduces friction.
A combination of muscles and tendons keeps your arm bone centered in your shoulder socket. These tissues are called the rotator cuff.
 Description
Description
Five major types of arthritis typically affect the shoulder.
Osteoarthritis
Also known as “wear-and-tear” arthritis, it is a condition that destroys the smooth covering (articular cartilage) of bone. As the cartilage wears away, it becomes frayed and rough, and the protective space between the bones decreases. During movement, the bones of the joint rub against each other, causing pain.
Osteoarthritis usually affects people over 50 years of age.
Rheumatoid Arthritis
Rheumatoid arthritis (RA) is a chronic autoimmune disease that attacks multiple joints throughout the body. It is many times symmetrical, meaning that it usually affects the same joint on both sides of the body. Shoulder can be affected as a part of rheumatoid arthritis.
The joints of the body are covered with a lining — called synovium — that lubricates the joint and makes it easier to move. Rheumatoid arthritis causes the lining to swell, which causes pain and stiffness in the joint.
Posttraumatic Arthritis
Posttraumatic arthritis is a form of osteoarthritis that develops after an injury, such as a fracture or dislocation of the shoulder.
Rotator Cuff Tear Arthropathy
Arthritis can also develop after a large, long-standing rotator cuff tendon tear. The torn rotator cuff can no longer hold the head of the humerus (ball) in the glenoid socket, and the humerus can move upward and rub against the acromion. This can damage the surfaces of the bones, causing arthritis to develop.
The combination of a large rotator cuff tear and advanced arthritis can lead to severe pain and weakness, and the patient may not be able to lift the arm away from the side.
Avascular Necrosis
Avascular necrosis (AVN) of the shoulder is a painful condition that occurs when the blood supply to the head of the humerus is disrupted. Because bone cells die without a blood supply, AVN can ultimately lead to destruction of the shoulder joint and arthritis.
Causes of AVN include high dose steroid use, heavy alcohol consumption, sickle cell disease, and traumatic injury, such as fractures of the shoulder. In some cases, no cause can be identified; this is referred to as idiopathic AVN.
Pain: The most common symptom of arthritis of the shoulder is pain, which is aggravated by activity and progressively worsens.
The pain is usually centered in the back of the shoulder and may intensify with changes in the weather. Patients complain of an ache deep in the joint.
Limited range of motion: Limited motion is another common symptom. It may become more difficult to lift your arm to comb your hair or reach up to a shelf. You may hear a grinding, clicking, or snapping sound (crepitus) as you move your shoulder.
As the disease progresses, any movement of the shoulder may cause pain. The pain may also disturb your sleep. Night pain is usually a symptom of advanced severity.
After discussing your symptoms and medical history, your doctor will examine your shoulder. He may request you to get some radiological and hematological (blood) investigations.
X-Rays
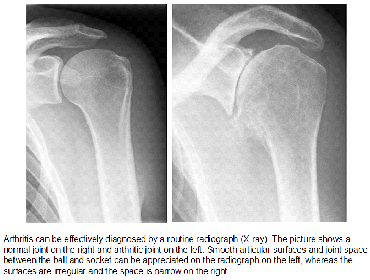
X-rays are imaging tests that create detailed pictures of dense structures, like bone. They can also help distinguish among various forms of arthritis.
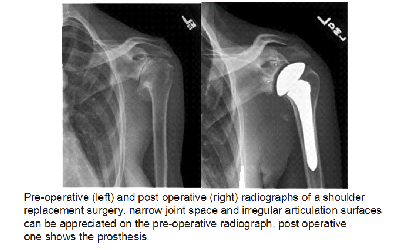
X-rays of an arthritic shoulder will show a narrowing of the joint space, changes in the bone, and the formation of bone spurs (osteophytes).
As with other arthritic conditions, initial treatment of arthritis of the shoulder is nonsurgical. Your doctor may recommend the following treatment options:
- Rest or change in activities to avoid provoking pain. You may need to change the way you move your arm to do things.
- Physical therapy exercises may improve the range of motion in your shoulder.
- Nonsteroidal anti-inflammatory medications (NSAIDs), such as aspirin or ibuprofen, may reduce inflammation and pain.
- Moist heat
- Ice your shoulder for 20 to 30 minutes two or three times a day to reduce inflammation and ease pain.
- If you have rheumatoid arthritis, your doctor may prescribe a disease-modifying drug, such as methotrexate.
- Dietary supplements, such as glucosamine and chondroitin sulfate may help relieve pain.
Please discuss the usefulness of drugs and their untoward actions with your shoulder surgeon before you start on any medications.
Joint injections:
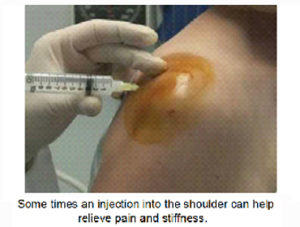
your surgeon may offer the option of injection into the shoulder joint. They may be sometimes injected under ultrasound guidance. There are many kind of injections, each having different functions. Some injections are intended to reduce pain and inflammation and others to lubricate the joint (viscosupplementation). Please discuss them with your surgeon.
If the pain is unrelenting even after Your doctor may consider surgery if your pain causes disability and is not relieved with nonsurgical options.
Arthroscopy: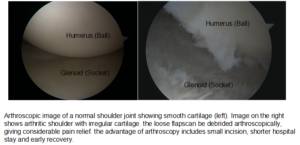 Cases of mild glenohumeral arthritis may be treated with arthroscopy, During arthroscopy, the surgeon inserts a small camera, called an arthroscope, into the shoulder joint. The camera displays pictures on a television screen, and the surgeon uses these images to guide miniature surgical instruments.
Cases of mild glenohumeral arthritis may be treated with arthroscopy, During arthroscopy, the surgeon inserts a small camera, called an arthroscope, into the shoulder joint. The camera displays pictures on a television screen, and the surgeon uses these images to guide miniature surgical instruments.
Because the arthroscope and surgical instruments are thin, the surgeon can use very small incisions (cuts), rather than the larger incision needed for standard, open surgery.
During the procedure, your surgeon can debride (clean out) the inside of the joint. Although the procedure provides pain relief, it will not eliminate the arthritis from the joint. If the arthritis progresses, further surgery may be needed in the future.
Shoulder joint replacement (arthroplasty): Advanced arthritis of the glenohumeral joint can be treated with shoulder replacement surgery, in which the damaged parts of the shoulder are removed and replaced with artificial components, called a prosthesis.
There are many types of replacement surgery of the shoulder:
Hemiarthroplasty. Just the head of the humerus is replaced by an artificial component.
Total shoulder arthroplasty. Both the head of the humerus and the glenoid are replaced. A plastic “cup” is fitted into the glenoid, and a metal “ball” is attached to the top of the humerus.
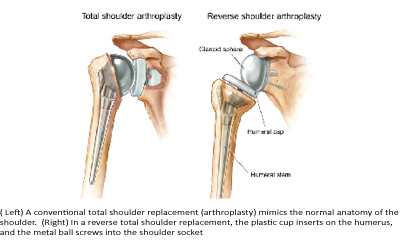
Reverse total shoulder arthroplasty. In a reverse total shoulder replacement, the socket and metal ball are opposite a conventional total shoulder arthroplasty. The metal ball is fixed to the glenoid and the plastic cup is fixed to the upper end of the humerus. A reverse total shoulder replacement works better for people with cuff tear arthropathy because it relies on different muscles — not the rotator cuff — to move the arm.
Recovery: Surgical treatment of arthritis of the shoulder is generally very effective in reducing pain and restoring motion. Recovery time and rehabilitation plans depend upon the type of surgery performed. You will generally spend a 2-3 weeks in an arm pouch following surgery, to rest your shoulder, following which rehabilitation exercises are started. Please discuss these with your surgeon.