


Anterior cruciate ligament injuries:
ACL surgery in bangalore is a medical procedure to supplant a torn anterior cruciate ligament (ACL) — a significant ligament in your knee. ACL wounds most regularly happen during sports that include unexpected stops and alters in course —, for example, basketball, soccer, football, downhill skiing and gymnastics. In ACL reconstruction, the torn tendon is removed and supplanted with a bit of ligament from another part of your knee or from a deceased contributor. This medical procedure is an outpatient method that is performed through little incisions around your knee joint. ACL recreation is performed by a specialist who works in surgeries of the bones and joints (orthopedic specialist).ACL surgery in bangalore
Anterior cruciate ligament(ACL) tear or sprain is one of the most common knee injuries, especially amongst the athletes. It can also very frequently happen during motor vehicle accidents. If you have injured your anterior cruciate ligament, you may require surgery to regain full function of your knee. This will depend on several factors, such as the severity of your injury and your activity level. The anterior cruciate ligament (ACL) is one of the most usually harmed tendons of the knee. Commonly the rate of ACL injury is higher in individuals who are associated with high-hazard sports, for example, ball, football, skiing, and soccer. Roughly 50% of ACL wounds happen in blend with harm to the meniscus, articular ligament, or different tendons. Also, patients may have wounds of the bone underneath the ligament surface. These might be seen on an attractive reverberation imaging (MRI) filter and may demonstrate injury to the overlying articular ligament. In this kind of critical situation, it becomes mandatory to undergo an ACL reconstruction surgery to come back for a normal situation. Because it is very difficult to perform any activity if you are not well from inside.
The knee joint is formed by three bones: The thighbone (femur), shinbone (tibia), and kneecap (patella). Bones are connected to one other and held in place by thick, rope like structures called ligaments. There are four primary ligaments in your knee and they are responsible to keep your knee stable.
Collateral ligaments
These are found on the sides of your knee. The medial collateral ligament is on the inside and the lateral collateral ligament is on the outside. They control the sideways motion of your knee and brace it against unusual movement.These are the ones found inside your knee joint. The ligament in front is the anterior cruciate ligament (ACL) and the one at the back is the posterior cruciate ligament (PCL). They cross each other to form an “X”. The cruciate ligaments control the back and forth motion of your knee.The anterior cruciate ligament prevents the tibia from sliding out in front of the femur. It also provides rotational stability to the knee.
 About half of all injuries to the anterior cruciate ligament occur along with damage to other structures in the knee, such as articular cartilage, meniscus, or other ligaments.
About half of all injuries to the anterior cruciate ligament occur along with damage to other structures in the knee, such as articular cartilage, meniscus, or other ligaments.
Injury to the ligaments are considered “sprains” and are graded on a severity scale.
Grade 1 Sprain: The ligament is mildly damaged in a Grade 1 Sprain. It has been slightly stretched, but is still able to help keep the knee joint stable.
Grade 2 Sprains: A Grade 2 Sprain stretches the ligament to the point where it becomes loose. This is often referred to as a partial tear.
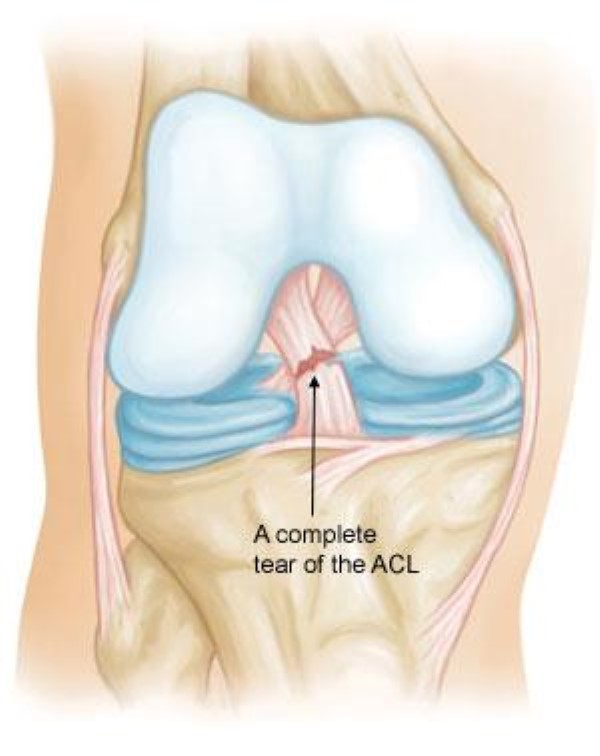
Grade 3 Sprains: This type of sprain is most commonly referred to as a complete tear of the ligament. The ligament has been split completely and the knee joint is unstable.
Partial tears of the anterior cruciate ligament are rare; most ACL injuries are complete or near complete tears.
Cause
The most common mechanism of anterior cruciate ligament injury is by a twisting injury to the knee. It can also be injured in several other ways:
- Sudden change of direction
- Stopping suddenly
- Slowing down while running
- Incorrect Landing from a jump
- Direct contact or collision, such as a football tackle
It has been shown in many studies that females have a higher incidence of ACL injury than male athletes in certain sports. This could be due to It has differences in physical conditioning, muscular strength, and neuromuscular control. Other suggested causes include differences in pelvis and lower extremity (leg) alignment, increased looseness in ligaments, and the effects of estrogen (hormone) on ligament properties.
When you injure your anterior cruciate ligament, you might hear a “popping” noise and you may feel a giving away sensation of your knee.
Other typical symptoms include:
- Pain with swelling: you may not experience swelling immediately, but usually Within 24 hours. If ignored, the swelling and pain may resolve on its own over a few weeks time. However, if you attempt to return to sports/ twisting or turning, your knee will probably buckle/ give way. This may cause further damage to the other structures inside the knee. So it is very important that you contact your surgeon and follow his advice, even though you feel comfortable a few weeks after the injury.
- Loss of full range of motion
- Tenderness along the joint line
- Discomfort while walking, especially on uneven surfaces.
- Doctor Examination
- Physical Examination and Patient History
- During your first visit, your doctor will talk to you about your symptoms and medical history.
- During the physical examination, your doctor will check all the structures of your injured knee, and compare them to your non-injured knee. Most ligament injuries can be diagnosed with a thorough physical examination of the knee. You doctor may request for imaging tests to confirm the diagnosis and also to make out if there are any other injuries.
Imaging Tests
X-rays: Although they will not show any injury to your anterior cruciate ligament, x-rays can show whether the injury is associated with a broken bone.
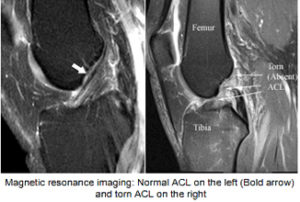
Magnetic resonance imaging (MRI) scan: This study creates better images of soft tissues like the anterior cruciate ligament. It also helps to diagnose any other associated injuries to other ligaments and cartilage in the knee.
A torn ACL does not heal on its own. Treatment for an ACL tear will depend upon the type of tear, the individual’s needs, occupation, age and sport. For example, the young individual with an active life style will most likely require surgery to safely return to sports. The less active, usually older, individual may be able to return to a quieter lifestyle without surgery.
Nonsurgical Treatment
A torn ACL will not heal without surgery. But nonsurgical treatment may be effective for patients who are elderly or have a very low activity level. If the overall stability of the knee is intact, your doctor may recommend simple, nonsurgical options.
Bracing: Your doctor may recommend a brace temporarily to protect your knee from buckling. To further protect your knee, you may be given crutches to keep you from putting weight on your leg.
Physical therapy. As the swelling goes down, a careful rehabilitation program is started. Specific exercises will restore function to your knee and strengthen the leg muscles that support it. You can get rid of the brace once you regain strength and balance in the knee.
Surgical Treatment
A torn ACL does not heal on its own and cannot be sutured (stitched) back together. To surgically repair the ACL and restore knee stability, the ligament must be reconstructed. During surgery, he torn ligament is replaced with a tissue graft. This graft acts as a scaffolding for a new ligament to grow on.
Grafts can be obtained from several sources.
1. patellar tendon: which runs between the kneecap and the shinbone.
2. Hamstring tendons: at the back of the thigh
3. Quadriceps tendon, which runs from the kneecap into the thigh, is used.
4. Cadaver donor graft (allograft)
The choice of the graft may depend on your age, activity, occupation, sport and finally familiarity of your surgeon. There are advantages and disadvantages to all graft sources. You should discuss the optimal graft choice for you with your knee surgeon to help determine which is best for you. Because the regrowth takes time, it may be six-nine months or more before an athlete can return to sports after surgery.
Procedure.
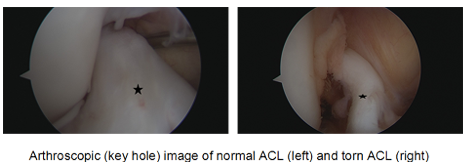
Surgery to rebuild an anterior cruciate ligament is done with an arthroscope (key hole surgery) using small incisions. The advantages of arthroscopic surgery is that it is less invasive. The benefits of less invasive techniques include less pain from surgery, less time spent in the hospital, and quicker recovery.

Whether your treatment involves surgery or not, rehabilitation plays a vital role in getting you back to your daily activities. A physical therapy program will help you regain knee strength and motion. If you have surgery, physical therapy first focuses on returning motion to the joint and surrounding muscles. This is followed by a strengthening program designed to protect the new ligament. The final phase of rehabilitation is tailored to suit your needs, occupation and sport. Most athletes can play cricket 6-9 months after surgery. Return to contact sports like football, basketball and martial arts may take anywhere between 9-12 months.
The following article provides in-depth information about treatment for anterior cruciate ligament injuries. The general article, Anterior Cruciate Ligament (ACL) Injuries, provides a good introduction to the topic and is recommended reading prior to this article. Success Story: ACL Surgery
What happens if I do not undergo surgery:
What happens naturally with an ACL injury without surgical intervention varies from patient to patient and depends on the patient’s activity level, degree of injury and instability symptoms.
Many patients are able to walk, climb stairs, go to the office and back even without an ACL. This is because ACL does not have much role with these activities. However, a few patients have buckling (instability) episodes even with activities of daily living. Most people will not be able to perform activities like running, jumping, twisting and turning, sudden change of direction. Playing contact sports will not be possible. Repeated buckling or instability episodes can cause injury to other structures in the knee like meniscus and cartilage. With chronic instability, a large majority of patients will have meniscus damage when reassessed 10 or more years after the initial injury. Similarly, the prevalence of articular cartilage lesions increases in patients who have a 10-year-old ACL deficiency. It may ultimately lead to arthritis.
Surgical Treatment
 ACL tears are not usually repaired using suture to sew it back together, because repaired ACLs have generally been shown to fail over time. Therefore, the torn ACL is generally replaced by a substitute graft made of tendon. There are multiple choices for graft that are available. The choice depends on your activity level, sport that you play, previously existing knee issues, occupation, concomitant injuries and many other factors. Few most commonly used graft sources are:
ACL tears are not usually repaired using suture to sew it back together, because repaired ACLs have generally been shown to fail over time. Therefore, the torn ACL is generally replaced by a substitute graft made of tendon. There are multiple choices for graft that are available. The choice depends on your activity level, sport that you play, previously existing knee issues, occupation, concomitant injuries and many other factors. Few most commonly used graft sources are:
- Patellar tendon autograft (autograft comes from the patient)
- Quadriceps tendon
- Hamstring tendon autograft
- Quadriceps tendon autograft
- Allograft (taken from a cadaver) patellar tendon, Achilles tendon, semitendinosus, gracilis, or posterior tibialis tendon
Timing of surgery:
Studies have shown that best results following ACL reconstruction are obtained if the surgery is delayed for a few weeks. This gives the best chance for inflammation to reduce. It also reduces the chance of arthrofibrosis (stiffness) following surgery. Discuss these in details with your knee surgeon before going through surgery.
During the waiting period, your surgeon may suggest icing, bracing and gentle exercises to aid in rehabilitation following surgery. This is called prehab and designed to help quicker recovery following surgery.
Surgical Procedure
Anaesthesia:
Decision regarding the type of anaesthetic is made collectively by the patient, the surgeon, and the anesthesiologist.
Surgery:
Graft preparation:
 The surgeon will harvest the appropriate graft and prepares it to insert into the knee. After the graft has been prepared, the surgeon places an arthroscope into the joint. Small (one-centimeter) incisions called portals are made in the front of the knee to insert the arthroscope and instruments and the surgeon examines the condition of the knee. Meniscus and cartilage injuries (if found) are trimmed or repaired and the torn ACL stump is then removed.
The surgeon will harvest the appropriate graft and prepares it to insert into the knee. After the graft has been prepared, the surgeon places an arthroscope into the joint. Small (one-centimeter) incisions called portals are made in the front of the knee to insert the arthroscope and instruments and the surgeon examines the condition of the knee. Meniscus and cartilage injuries (if found) are trimmed or repaired and the torn ACL stump is then removed.
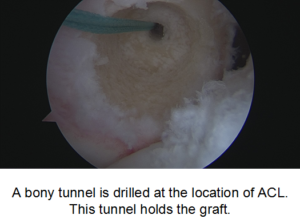 In the most common ACL reconstruction technique, bone tunnels are drilled into the tibia and the femur to place the ACL graft in almost the same position as the torn ACL.
In the most common ACL reconstruction technique, bone tunnels are drilled into the tibia and the femur to place the ACL graft in almost the same position as the torn ACL.
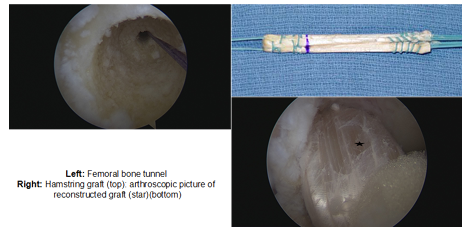
The graft is pulled into position up through tunnels. The graft is held under tension as it is fixed in place using interference screws, spiked washers, posts, or staples. The devices used to hold the graft in place are generally not removed. There are many kinds of fixation devices available, some of which are bio-degradable (dis-integrates in the body). Discuss the options with your knee surgeon before making the decision.
Once the surgery is done, the wound is closed and dressing is applied. Your surgeon may place your limb in a brace. The patient will usually go home on the same day of the surgery.
Pain Management
After surgery, you will feel some pain. This is a natural part of the healing process. Your doctor and nurses will work to reduce your pain, which can help you recover from surgery faster.
Your surgeon may infiltrate your knee with local anaesthetic mixture at the end of surgery. This reduces post operative pain and swelling. Medications are often prescribed for short-term pain relief after surgery. Many types of medicines are available to help manage pain, including opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and local anesthetics. Your doctor may use a combination of these medications to improve pain relief, as well as minimize the need for opioids.
Rehabilitation
Physical therapy is a crucial part of successful ACL surgery, with exercises beginning immediately after the surgery. Much of the success of ACL reconstructive surgery depends on the patient’s dedication to rigorous physical therapy. With new surgical techniques and stronger graft fixation, current physical therapy uses an accelerated course of rehabilitation.
Postoperative Course. In the first 10 to 14 days after surgery, the wound is kept clean and dry, and early emphasis is placed on regaining the ability to fully straighten the knee and restore quadriceps control.
 The knee is iced regularly to reduce swelling and pain. The surgeon may dictate the use of a postoperative brace and the use of a machine to move the knee through its range of motion. Weight-bearing status (use of crutches to keep some or all of the patient’s weight off of the surgical leg), bracing is also determined by physician preference, as well as other injuries addressed at the time of surgery.
The knee is iced regularly to reduce swelling and pain. The surgeon may dictate the use of a postoperative brace and the use of a machine to move the knee through its range of motion. Weight-bearing status (use of crutches to keep some or all of the patient’s weight off of the surgical leg), bracing is also determined by physician preference, as well as other injuries addressed at the time of surgery.
Rehabilitation: The goals for rehabilitation of ACL reconstruction include reducing knee swelling, maintaining mobility of the kneecap to prevent anterior knee pain problems, regaining full range of motion of the knee, as well as strengthening the quadriceps and hamstring muscles.
The patient may return to sports when there is no longer pain or swelling, when full knee range of motion has been achieved, and when muscle strength, endurance and functional use of the leg have been fully restored. The patient’s sense of balance and control of the leg must also be restored through exercises designed to improve neuromuscular control.
Most surgeons allow stationery cycling and swimming between 2-3 weeks following surgery. Gentle jogging can be started at 3 months. Playing golf is usually allowed 3-4 months after surgery, where as cricket at 6 months and football and basketball between 8-9months.
The use of a functional brace when returning to sports is ideally not needed after a successful ACL reconstruction, but some patients may feel a greater sense of security by wearing one.